

The goals of the TFOS DEWS II Definition and Classification Subcommittee were to create an evidence-based definition and a contemporary classification system for DED.
A review of the history behind our understanding of dry eye helps place this most recent revised definition of DED in context. Dry eye became formally defined as a disease state only a little over 30 years ago. By the early to mid-1990s, understanding of dry eye had reached a critical point, with the field poised and eager for rapid development. The first definition of dry eye, published in 1995 on the basis of consensus from the NEI/Industry working group on Clinical Trials in Dry Eye, was as follows [2].
‘‘Dry eye is a disorder of the tear film due to tear deficiency or excessive tear evaporation which causes damage to the interpalpebral ocular surface and is associated with symptoms of ocular discomfort.”Importantly, this early definition identified the relevance of tear film quality as well as tear quantity as a cause of dry eye. For many, the 1995 definition and report provided a blueprint for clinical, translational, and basic research that would propel the field to the next level. Of note is that the definition used the term “disorder” and not “disease”.
Along similar lines, in 2006, a Delphi consensus group proposed a new name for DED, reflecting the relevance of both tear quality and quantity, namely ‘dysfunctional tear syndrome’. A classification system was similarly created designed to guide treatment based on disease with or without clinically evident inflammation [3].
In 2007, the first TFOS DEWS definition of dry eye was published, following a three-year international consensus-based process [4]. Scarcely 10 years after the publication of the initial NEI/Industry report, significant advances in dry eye had been made. The growing body of literature, and increased focus on diagnostics and therapeutic approaches, led to a revised definition that centered on the clinical effects and associated signs [4].
The original TFOS DEWS workshop was the first to acknowledge that dry eye was indeed a disease entity, with a multifactorial etiology. Again, symptoms were acknowledged to be paramount, but were noted to include not only discomfort symptoms but also symptoms of transient visual disturbance. While the sequelae of dry eye were described in terms of symptoms and tear film instability, and that increased tear film osmolarity and inflammation accompanied the disease, a statement regarding the mechanism or etiology of DED was not included. Specifically, increased osmolarity and inflammation were described as casual and not causal markers of the disease.
Following preliminary subcommittee discussions, a survey of the TFOS DEWS II membership, conducted in late 2015, asked specifically whether the original DEWS definition was acceptable and should remain as the DEWS II definition. Of those who responded, 77% voted for the definition to be changed. In forced choice questioning, support was indicated for a simplified definition, or truncated version of the original, DEWS definition, however almost 2/3 of the membership provided additional feedback, noting specific concerns.
Specifically, it became clear that TFOS DEWS II members acknowledged the significant role of inflammation and hyperosmolarity within the DED pathway, but challenged inclusion of those precise terms in the definition, due to a perception that clinical demonstration of these pathophysiological features was required to validate a diagnosis of dry eye. To address this, and other concerns, a group of representatives from the Definition and Classification Subcommittee, the Harmonization and Steering Committee, met in December 2016 in St. Paul, MN (USA), following review of all submitted TFOS DEWS II reports, to finalize the definition proposed by the Definition and Classification Subcommittee.
A number of critical points were discussed, including acknowledgement that a loss of tear film homeostasis can arise from a multitude of factors that encompass eyelid and blink abnormalities, in addition to ocular surface or tear component deficiencies [1,5]. These changes can induce focal or global tear film instability and tear hyperosmolarity in response to excessive evaporation from the ocular surface, and are regarded as significant entry points that contribute to the pathogenesis and perpetuation of a cycle of events, or “Vicious Circle”, in DED [4,6,7]. As characterizing the precise interactions within this complex ocular surface and tear film environment is challenging, it was deemed valuable to include both the expected outcome of the disease (a clinically measurable disruption of tear film homeostasis) as well as highlight key etiological elements in the definition. The etiological elements are important in maximizing specificity in defining dry eye, to differentiate it from other ocular surface diseases. The breadth of potential changes that might occur under the umbrella of homeostatic imbalance allows the clinician, researcher, industry representative, and/or regulatory body the autonomy to select the features most appropriate as outcome measures in accordance with the specific dry eye etiology under investigation. The focus on crafting a definition and classification with sufficiently broad interpretation to allow for growth and flexibility in the field of dry eye research remained paramount throughout the definition development process.
Emerging over the last decade has been mounting evidence of the potential role of neurosensory abnormalities in the understanding and management of DED. Neuropathic pain occurs due to overt damage within the somatosensory nervous system, distinguishing it from DED. Nociceptive pain occurs in response to local tissue damage. Corneal nociceptors, which transmit somatosensory “pain” information to the central nervous system, have the potential to be sensitized by repeated physiological stimulation or by noxious stimuli (e.g., hyperosmolarity or inflammation) [8]. While a comprehensive understanding of the exact role that neurosensory abnormalities play within the pathophysiological pathways of DED is yet to be reached, their potential, while we await elucidation by further study, is deemed worthy of recognition.
Clinically, dry eye is often described as ‘chronic’ and ‘progressive’, although there is currently insufficient evidence to support inclusion of these terms in the definition. While omission of these terms from the definition is warranted at present, additional research, including dry eye natural history studies, should be performed to inform future refinements to the definition terminology.
Thus, in summary, the TFOS DEWS II membership, on the basis of current evidence, acknowledged that the definition needed to recognize the multifactorial nature of DED, and there was agreement that the unifying element in DED is the loss of homeostasis of the tear film. Ocular symptoms, which include discomfort or visual disturbance, or both, remain a central feature of the disease. Conveying the key etiological roles of tear film instability, hyperosmolarity, ocular surface inflammation and damage was deemed valuable in recognition of the cyclical disease process, with its various entry points, as described in the Pathophysiology and Tear Film reports [1,5]. Acknowledging the role that neurosensory abnormalities play in the etiology of the disease was also considered worthy of inclusion within the definition, in light of the expanding literature in this area [8].
This process led to the refined TFOS DEWS II global dry eye definition, as follows:
The terminology used in the definition, including diction, word order, emphasis, and accepted meaning were deemed critical in creating an internationally accepted definition suitable for translation to multiple languages. The individual terms are described in turn.
The 2007 DEWS report recognized dry eye as a complex, multifactorial disease that cannot be characterized by a single process, sign or symptom. In medical terms, multifactorial is described as having, or stemming from, a number of different interacting causes or influences, as is the case in DED.
Since 2007, the definition has recognized dry eye as a disease. Although definitions of ‘disease’ vary, it is generally understood to be a disorder of structure or function or a condition of illness that results in specific signs or symptoms. From a patient care perspective, as well as providing global appreciation of dry eye as an entity with pathologic and quality of life implications, it was considered important to retain the term “disease” in the definition [9].
For the purposes of this definition, in alignment with previous TFOS reports [4,10,11], the ocular surface is defined as comprising the structures of the eye and adnexa, including the cornea, conjunctiva, eyelids, eyelashes, tear film, main and accessory lacrimal glands, and the meibomian glands. Thus, the tears, both in terms of the individual components at the site of production, and as a film on the ocular surface, are included within the term “ocular surface.”
The tear film has a vital role in providing lubrication and protection to the ocular surface, as well as maintaining a smooth, refractive surface for optimal visual performance [5]. Physiologically, homeostasis describes the state of equilibrium in the body with respect to its various functions, and to the chemical composition of the fluids and tissues [12]. When applied to DED, the concept of disrupted tear film homeostasis acknowledges the possibility of the many different changes that can occur in the tear film and ocular surface [5], in response to one or more of the underlying causes of dry eye [1]. Disruption of homeostasis is considered to be the unifying characteristic that describes the fundamental process in the development of DED.
The 1995 definition of dry eye identified discomfort as the principal symptomatic response associated with dry eye [2], and the 2007 definition expanded the concept of symptoms to include visual disturbance. While terminology varies with language and between different cultures, for example, the terms ‘gritty eyes’ or ‘stinging eyes’ are not frequently reported or understood in Mandarin [13], ocular symptoms remain a fundamental component of DED. The original TFOS DEWS report retained discomfort as a term within the definition, but expanded the concept of symptoms to include visual disturbance, in acknowledgement of the transient blurring reported by affected individuals that corresponded with disrupted tear surface quality [4]. TFOS DEWS II concedes that both discomfort and visual disturbance symptoms remain fundamental to DED, but to avoid restriction and maximizing relevance across the world, has chosen the phrase “…accompanied by ocular symptoms” for the current definition, to encompass a broader range of possible symptoms associated with DED.
The term “etiological role” emphasizes the concept of an involved pathway, without suggestion that specific features be considered as measurement outcomes or required diagnostic elements.
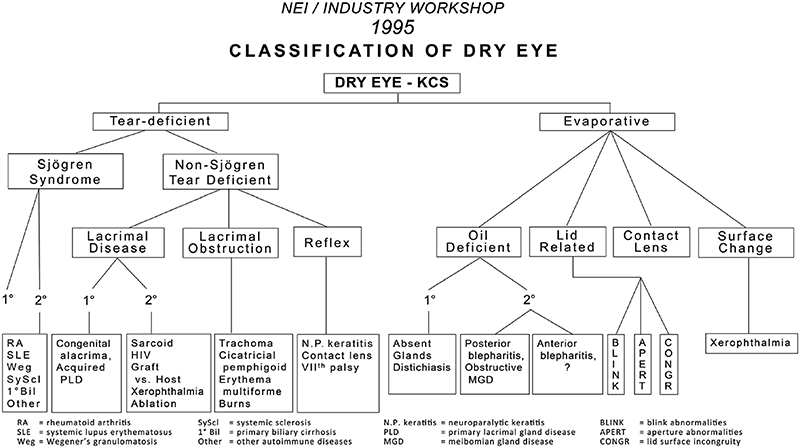
Dry eye classification schemes serve to guide diagnosis and ultimately improve patient care through appropriate treatment. The NEI/Industry Report (Fig. 1) [2] identified the two primary categories of dry eye as tear deficient and evaporative, and proposed, in sub-classification, a range of intrinsic and extrinsic etiological factors believed to contribute to dry eye development within these categories.
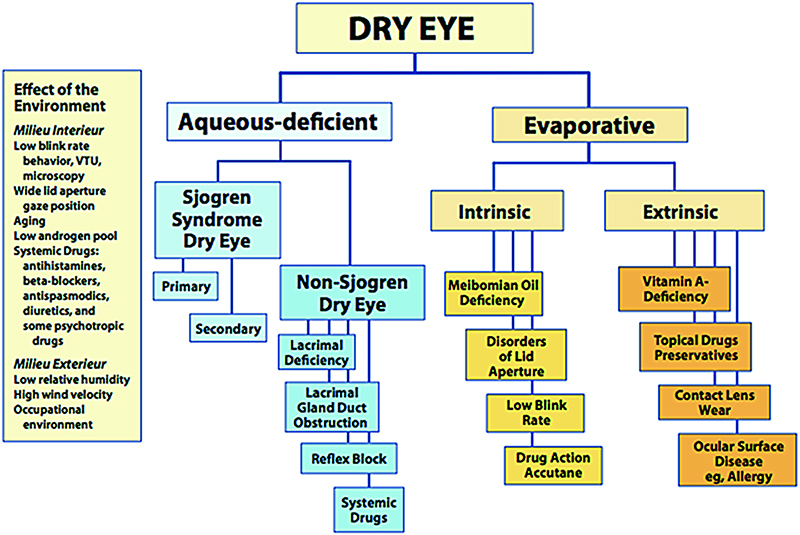
The classification scheme presented by the TFOS DEWS report (Fig. 2) retained the two primary categories, aqueous deficient and evaporative, although ‘tear deficient’ was redefined more specifically as ‘aqueous deficient’ [4]. Once again, possible disease etiologies were listed in a sub-classification tree.Fig. 2
During the TFOS DEWS II process a number of issues with the interpretation of the original DEWS classification scheme were highlighted. The first related to the distinction between the primary categories of dry eye. Co-existence of deficiencies in both tear quantity and quality are not uncommon as a result of the cyclical, self-perpetuating nature of DED. Once an individual enters into the ‘Vicious Circle’, irrespective of the entry point, the ensuing tear film instability, hyperosmolarity, and inflammation serve to drive further adverse change, often blurring the distinction between underlying aqueous deficient and evaporative etiologies [1].
While potential overlap between the aqueous deficient and evaporative categories had been acknowledged in the original DEWS report [4], both in the text and in the schematic representation of the pathophysiological process, the classification scheme was perceived by many to convey a sense of mutual exclusivity by depicting the aqueous deficient and evaporative categories as distinct. While the last decade of scientific evidence indicates that the fundamental understanding has not shifted dramatically since DEWS, it became apparent that addressing the common misconception associated with the classification scheme, by ensuring the potential for overlap between these two categories was discussed, would be important in TFOS DEWS II.
A second issue arose concerning the accuracy of placement of some conditions within the DEWS sub-classification zone. The purpose of including concurrent sub-class presentations had been to aid clinicians in deriving an appropriate management plan. However, recent evidence has suggested that a number of conditions could arguably be listed under more than one heading. For example, Sjögren syndrome, which, in the 1995 and 2007 reports [2,4] was classified exclusively as being due to aqueous deficiency, has become increasingly recognized to possess, concurrently, an evaporative component, due to associated meibomian gland dysfunction (MGD) [14] that impacts predominantly upon tear-lipid function.
Additional concern surrounded the level of specificity important in DED diagnosis to avoid misdiagnosis of other ocular surface diseases as DED. Such non-specificity in diagnosis increases the risk of perceived treatment failure, resulting not only in disillusioned patients and clinicians, but threatening the outcomes of clinical trials and regulatory approval of novel therapies, through insufficiently precise inclusion criteria.
The current report attempts to remove any perception of exclusivity in the classification of dry eye by indicating in the scheme that aqueous deficient and evaporative dry eye diagnoses exist on a continuum rather than as separate entities. In diagnosis [15], and in management [16], elements of each should be considered.
This dry eye classification scheme incorporates triaging elements to provide clarity in diagnosing DED (via the Diagnostic Methodology report) [15], from which the various etiologies can be considered (see Pathophysiology report) [1] and an appropriate management plan can be instituted (see Management and Therapy report) [16]. Appropriate management of differentially diagnosed ocular surface conditions that masquerade as DED increases the chances of successful treatment and allows any co-existing component of the condition attributable to DED to be revealed and suitably managed.
Sub-classification is recommended to be undertaken with reference to the TFOS DEWS II Pathophysiology report [1], which describes the wide range of possible DED subcategories and alludes to their predominant etiology within the aqueous deficient and evaporative continuum. Importantly, based on the evidence summarized in the various TFOS DEWS II reports, the classification scheme also considers the cases where patients exhibit dry eye symptoms without evidence of obvious signs, or present with marked signs but are absent of dry eye symptoms [8,17].
Fig. 3 incorporates a clinical decision algorithm, based on the current knowledge of the pathophysiology of DED, which seeks to promote accuracy in the classification of potential DED presenting to the eye care practitioner.

As with the definition of DED, a detailed description of the terminology is provided to clarify the decision-making behind the development of the classification scheme. In the following section, specific elements in the 2017 dry eye classification (Fig. 3) are introduced and described.
Over twenty years of research and countless patient encounters have promoted evolution of the understanding of DED. In alignment with the definition, the DED classification recognizes the necessity of symptomatic involvement and the presence of associated ocular surface signs in making a diagnosis of DED. For the classification scheme presented here, DED is differentiated from other ocular surface diseases, as well as in instances where there are symptoms and no signs, or signs and no symptoms.
Ocular surface disease is the broad category that is considered to include a multitude of ocular surface conditions, some of which closely mimic or masquerade as DED, and many that can occur concurrently with DED [15]. Because of this complexity and overlap, dry eye is frequently treated as a diagnosis of exclusion. The TFOS DEWS II Diagnostic Methodology report presents “triaging questions” [15], which can be used, in combination with clinical findings, to differentially diagnose other ocular surface conditions that may require specific management, and result in relief of signs and symptoms that might otherwise be attributed to DED.
It is important to note that many ocular surface diseases can be co-morbid with dry eye, thus a step-wise approach to management, with subsequent follow-up to monitor signs and symptoms is warranted. For example, symptoms and tear film changes commensurate with DED might well occur in a condition such as lagophthalmos, due to poor lid to globe apposition, preventing formation of a stable inter-blink tear film. However, resolution with dry eye therapies alone is unlikely to succeed, as the surfacing problem cannot be resolved without managing the lagophthalmos. The converse of this scenario is that restoration of lid-globe apposition through surgical management of the lagophthalmos has the potential to fully resolve the dry eye symptoms and signs without the need for dedicated dry eye therapies [16,19]. Further research is needed regarding co-morbid ocular surface conditions that induce a “secondary” dry eye.
The Pain and Sensation Subcommittee report describes a clinical scenario of neuropathic pain due to either a lesion or disease in the somatosensory system, in which ocular pain symptoms disproportionally outweigh the clinical signs [8]. This is an important distinction in the diagnosis, and the required pain management falls outside the scope of DED therapy [8].
It is further recognized that symptoms consistent with DED, but in the absence of clinical signs, especially when the symptoms are intermittent, might indicate a pre-clinical dry eye state, or a scenario of emerging episodic dry eye. Ongoing evaluation for the development of signs and the control of symptoms through education and prevention are suggested. Studies evaluating the natural history of short and long-term preventative efforts in this patient group are needed [9]. Determination of whether such individuals are at higher risk of developing iatrogenic DED, in comparison to those who are non-symptomatic, is also deserving of further investigation [17].
Patients exhibiting signs of ocular surface disease, but reporting no symptoms of discomfort, require consideration of whether dry eye management is indicated. Corneal nerve damage secondary to longstanding DED is a recognized phenomenon and the reduced corneal sensitivity can mask discomfort. The dysfunctional sensation is a function of the underlying disease process. Other forms of corneal disease exist, where corneal sensation is reduced, and these should also be managed accordingly [17].
Ocular surface changes in the absence of presenting symptoms may be noted during a preoperative examination for cataract or refractive surgery, for example, and signify early disease that might place the patient at risk of developing symptomatic DED following the surgical event [17]. Preventative management should be considered, as described in more detail in the Iatrogenic report [17]. Recently, asymptomatic MGD has been reported with a prevalence of double that of symptomatic MGD in a Caucasian population [20]. While there are limited data on the natural history of DED, symptoms do become more common with age [9] and individuals with MGD are more likely to report an increase in severity of their symptoms with time [21], all of which may support an argument for intervention.